Arterial Disease
Diseases of the arterial system can be broadly divided into Occlusive Vascular Disease (blockages) and Aneurysmal Disease (enlargements).
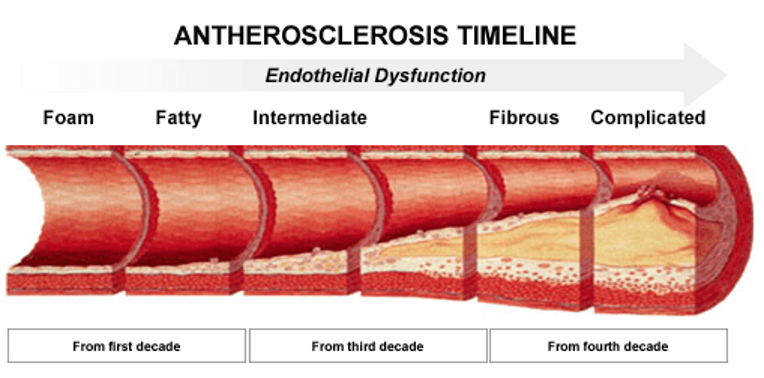
- Occlusive Vascular Disease – a build up of atherosclerosis (hardening of the arteries) occurs in all humans over time. However, certain risk factors help to promote the formation of arterial plaque:
- Smoking
- Hypertension
- Hypercholesterolemia
- Diabetes
- Family History (genetics)
Of these risk factors, smoking remains the most powerful promoter of arterial occlusive disease
The clinical manifestations related to occlusive disease range from no symptoms (the vast majority of us) to exercise-induced muscle pains and finally to limb-threatening lack of blood supply that can lead to potential limb loss. Progression of this disease process is usually slow and steady, however, is some circumstances acute (sudden) arterial blockages can occur resulting in potential limb loss. Vascular Surgeons largely deal with the progression of Arterial Disease in the neck (carotid arteries), arms, chest, abdomen and legs. A Vascular Surgeon deals with all arterial disease outside of the heart itself.
By far the most common clinical presentation is termed Intermittent Claudication. Claudication is defined simply as a ‘lame leg’. In the context of occlusive vascular disease it typically occurs after a period of exercise. In basic terms the blockages that have built up over time do not allow exercising muscle groups to be supplied with an appropriate amount of arterial blood supply. This results in the build up of lactic acid in the affected muscle groups. This causes achy muscle pain. The pain is relieved by a short period of rest and the patient can then resume activity. While this pain certainly can be lifestyle limiting, it is not limb threatening at this stage.
The differential diagnosis of this problem includes:
- Degenerative disc disease
- Osteoarthritic joint disease
Your Vascular Surgeon is highly trained to differentiate between these disease processes using history, clinical exam and both non-invasive (doppler) and more invasive (angiography) tests.
Typical treatment of Intermittent Claudication includes life style modifications (smoke cessation and a walking program) as well as the use of antiplatelet medications (aspirin, clopidogrel) and a cholesterol lowering agent. These simple interventions can stabilize the disease process and allow time for alternative arterial branches (collaterals) to form. In the majority of patients, these simple measures may be all that is required. Your physician may monitor the burden of disease with non-invasive tests (Arterial Doppler studies) on a regular basis.
In some situations these basic conservative measures are not adequate to relieve the discomfort associated with this disease process. Therefore a number of surgical interventions are possible to help relieve the burden of disease.
The most common interventions include:
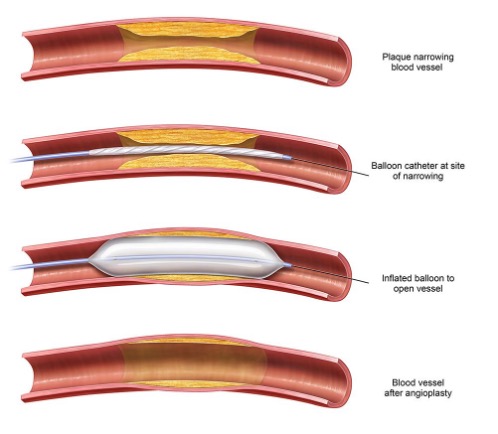
- Balloon Angioplasty – this means dilating the area of narrowing (stenosis) with a balloon to relieve the narrowing.
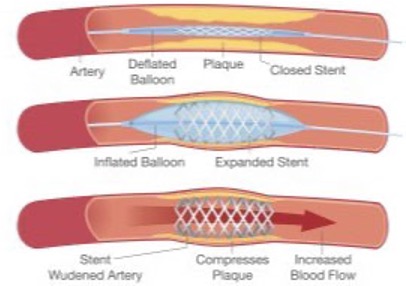
- Angioplasty and Stenting – the act of angioplasty distends the artery and actually causes a small trauma to the vessel. Your body responds with a healing (inflammatory) response that can lead to scarring of the artery where the angioplasty was performed. The idea behind stenting is to try to defeat the re-narrowing scar formation by placing a structure (usually metal) that supports the artery around the angioplasty site.
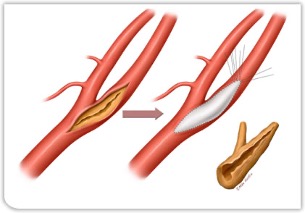
- Endarterectomy – this term means that the plaque is removed from the artery and the artery is repaired. This is an excellent treatment for large localized plaques that may not be amenable to balloon angioplasty. Common areas where this is utilized is in the Carotid Artery and Femoral Artery.
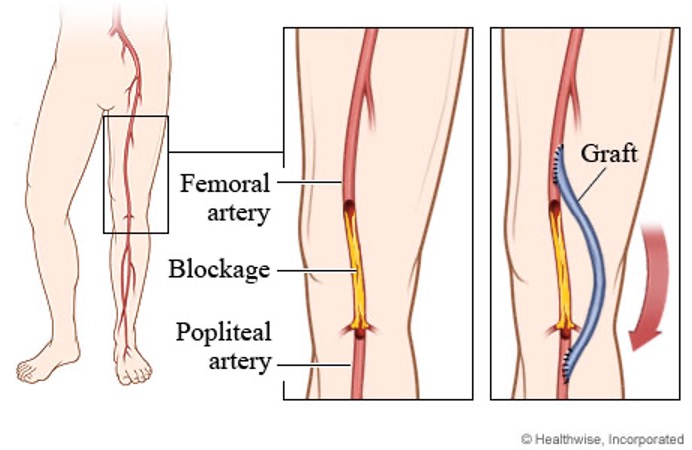
- Arterial Bypass Surgery – when the arterial disease burden is so significant that angioplasty is no longer feasible or potentially has a poor long term result, arterial reconstruction with a bypass is the best treatment choice
Vascular Surgeons are fully trained to deliver all of these potential treatment options and will help you to choose the most effective means of treating the problem. The treatment choice involves an overall risk assessment as well as a detailed assessment of your disease burden. The goal of treatment is to always try to optimize the clinical outcome for a patient.
- Aneurysmal Disease – an aneurysm is defined as a localized dilatation of a blood vessel beyond twice normal size in greatest diameter.
The most common site for an arterial aneurysm is the Abdominal Aorta. The Aorta is the largest artery in the human body. The average normal diameter of this vessel is approximately 1.5 to 2.0 cm. An aneurysm is therefore at least 3.0 cm in diameter.
The cause of aneurysmal change to the aorta is still not fully understood. However, certain inheritable (genetic) causes are related to aneurysmal change. The most common of these include Marfan’s Syndrome and Ehler’s Danlos Syndrome. These genetic traits predispose patients to aneurysmal change based on inborn errors of connective tissue formation. Most patients with aneurysms do not have a recognizable genetic history of these problems. However, there is a close association between a history of smoking and aneurysmal change in the aorta. Other causes of aneurysms include hypertension, traumatic injuries and infectious causes.
Aneurysms can cause a number of problems including rupture, thrombosis, embolization, compression of adjacent structures, and erosion into surrounding structures. The most common and dramatic complication of an abdominal aortic aneurysm is rupture. This is a life threatening condition that is fatal if untreated.

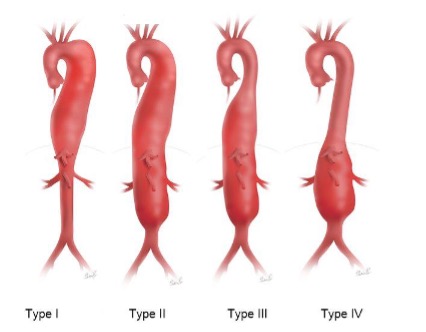
Some Aortic Aneurysms are more extensive with involvement of long segments of the main blood vessel and its branches. These are termed Thoracoabdominal Aortic Aneurysms because they involve the aorta both in the chest (thorax) and the abdomen.
Treatment for Aortic Aneurysms in the absence of symptoms is recommended after the aneurysm reaches at least 5.5cm in diameter in men and 5.0 cm in women. However, due to the nature of this type of this disease process, risks are involved both with and without treatment and each patient is carefully evaluated by their Vascular Surgeon to achieve the best possible outcome. A full evaluation will include a careful history and physical, arterial duplex assessment, contrast imaging (CT scan) and a cardiac assessment. The purpose of treatment is to prevent aneurysm rupture and therefore lengthen the patient’s life span.
Treatments for aneurysms include:
- Open Aneurysm Repair
- Endovascular Aneurysm Repair
- Hybrid (open plus endovascular) Aneurysm Repair
All of these treatments have associated risks and benefits. The role of the Vascular Surgeon is to carefully evaluate both the patient and their arterial anatomy to determine the optimal approach. In younger, healthier patients or those with genetic traits, open surgery is usually the desired approach. In older patients with suitable anatomy less invasive approaches may be the best option. All patients are evaluated for both open and endovascular approaches. The goal of treatment is to provide the best possible outcome for each patient using whatever approach is deemed to be the most beneficial to the patient. Vascular Surgeons have extensive training in all approaches to aneurysmal disease.
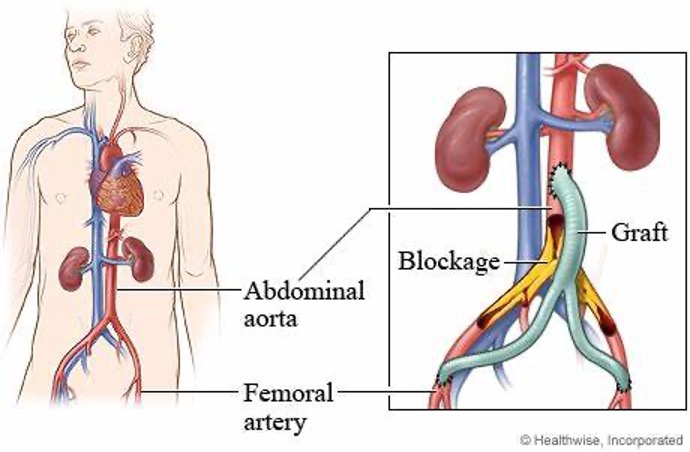
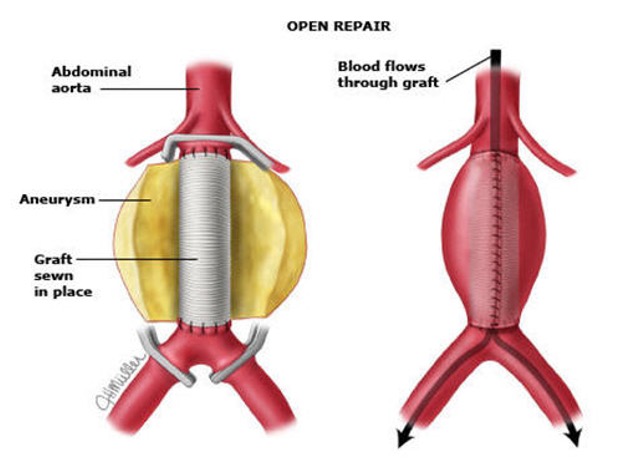
Open Aneurysm Repair
Open surgery has existed since the mid 1950’s. It involves a long abdominal incision and direct repair of the affected artery. The artery is replaced by a graft material (usually Dacron (knitted polyster)) that is very durable, is hand sewn by the surgeon, and should last the for the rest of the patient’s life.
Typically this involves a general anesthetic and a hospital stay of about 5-7 days. Healing of the incision requires about 6-8 weeks. During the healing time, he patient is fully mobile but is cautioned to not exercise to vigorously to allow the incision to heal and prevent a hernia from forming.
Once healed, this is typically a ‘one of’ procedure and lost patients resume their normal life and are followed annually with a duplex study of the graft.
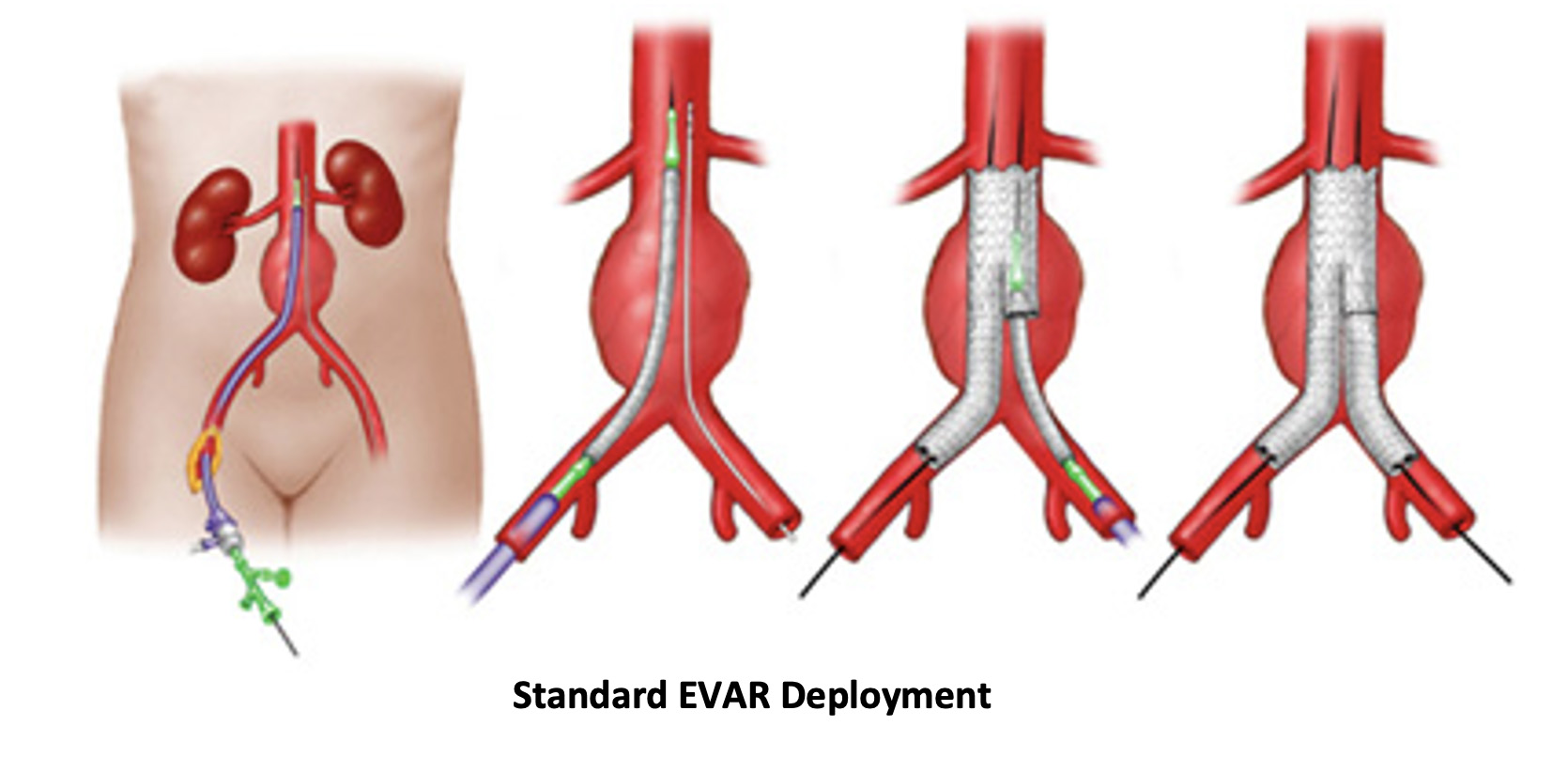
Endovascular Aneurysm Repair (EVAR)
EVAR is a modality that has existed in various forms for about 20 years.
It involves deploying a device on the inside of the aneurysm to divert flow away from the arterial wall and therefore decompress the aneurysm from the inside out. The device is held in place with small hooks and barbs and requires certain well-studied anatomic ‘landing zones’ to enable long term success of the device deployment
The advantage of EVAR is that patients recover much faster because there is no large abdominal incision. This procedure is performed through small incisions in both groins and can even be performed just through large needle punctures that can be sealed without an incision. This is of course very appealing to patients and surgeons alike.
However, not all patients are anatomically suitable to this type of repair. In addition, aneurysmal disease is slowly progressive, therefore the landing zones can change over time and this may affect the long term outcome associated with this form of repair. EVAR requires careful, regular follow-up post-op for the life of the patient to ensure that the device remains effective.
A Vascular Surgeon carefully evaluates the patients characteristics both anatomically and medically to arise at the correct treatment choice.